652
Facility TB Diagnoses
Bungoma County, Kenya | January-November 2024

Official Document | AIGHAP Impact Brief Repository
The African Initiative for Global Health, Advocacy, and Policy (AIGHAP) implemented the TB CRG Wave 11 grant under the auspices of Stop TB Partnerships Kenya between January and November 2024. AIGHAP sought to increase participation, accountability, non-discrimination, empowerment, linkage, and sustainability among vulnerable and marginalized populations affected by TB in Bungoma, Kenya, through PANELS for TB in Kenya (PANELS K). The program deployed 20 TB champions and one coordinator across 10 health facilities in six subcounties, and assessed performance pre-implementation (2023) and during implementation (2024, January-September).
Between 2023 and 2024, community-facility case-finding activities screened 145,575 individuals, resulting in 652 confirmed TB diagnoses and 652 treatment initiations. Community TB champions enabled 306 diagnoses, representing 46.9% of all detected cases. The program recorded a diagnostic yield of 10.3%, number needed to screen (NNS) of 372.3, and number needed to test (NNT) of 9.7.
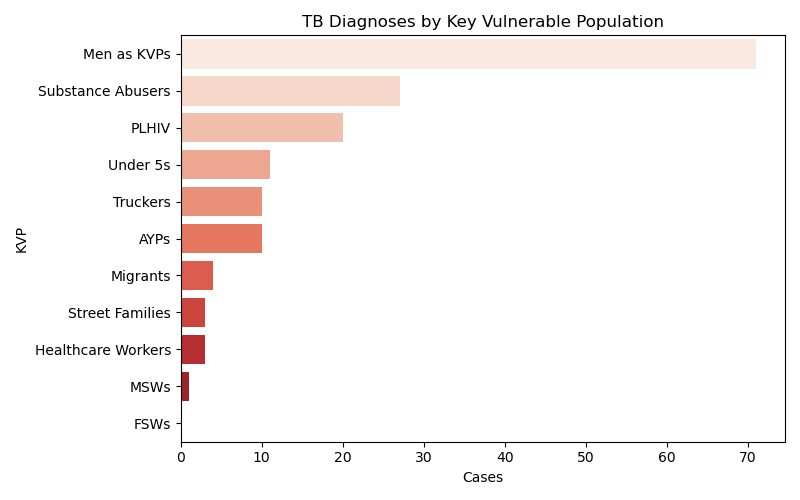
Community outreach reached transport corridor workers, substance users, migrants, prisoners, and other underserved populations. Geographic and facility analyses identified key diagnostic hotspots, and the overall detection rate reached 447.9 TB cases per 100,000 screened. Findings show that integrating trained TB champions into community health systems strengthens early detection, community-facility linkage, and TB notification among vulnerable populations.
Across 10 integrated facilities, TB champions were institutionally embedded as supervised community-facility actors. This integration improved symptom screening, referral completion, and treatment linkage by combining facility workflow discipline with hotspot intelligence.
Diagnostic cascade tracking demonstrated strong continuity from screening through treatment initiation. No diagnosed client was lost before treatment start, signaling robust coordination between outreach, triage, and clinical teams.
Champion contribution scaled across implementation, increasing from 23.7% in January to 47.7% in April and sustaining 46.9% in May. This trend indicates progressive normalization of champion-led diagnostic support inside routine operations.
The rights and vulnerability lens remained central to delivery. Men in hotspot zones faced delayed care due to alcohol dependency and unstable income, while women and girls reported stigma, GBV-linked constraints, food insecurity, and psychosocial pressure affecting adherence.
Adolescents and youth encountered school-based stigma and continuity barriers, while substance-dependent populations faced interruption risks associated with homelessness and food insecurity. Support groups functioned as practical adherence and stigma-reduction platforms.
Despite delayed operational clearance and strike disruption, a $50,000 grant produced 306 champion-enabled diagnoses (about $163 per diagnosis), indicating strong value-for-investment under constrained implementation conditions.
Structured Diagnostic Acceleration Framework: Embeds trained community actors into facility diagnostic workflows; accelerates case detection; preserves cascade integrity; institutionalizes integration.

| Total workload | 184,179 |
| Individuals screened | 145,575 |
| Presumptive TB cases | 4,534 |
| Individuals evaluated | 2,845 |
| TB cases diagnosed | 652 |
| Treatment initiations | 652 |
| Champion-enabled diagnoses | 306 |
| Champion contribution (%) | 46.9 |
| Champion productivity (cases/champion) | 14.6 |
| Screened (cascade sample) | 644 |
| CXR triage | 436 |
| Investigated | 266 |
| Diagnosed | 26 |
| Initiated treatment | 26 |
| Diagnostic yield (%) | 10.3 |
| Number needed to screen (NNS) | 372.3 |
| Number needed to test (NNT) | 9.7 |
| Bacteriological confirmation (%) | 44.9 |
| Detection rate (per 100,000 screened) | 447.9 |
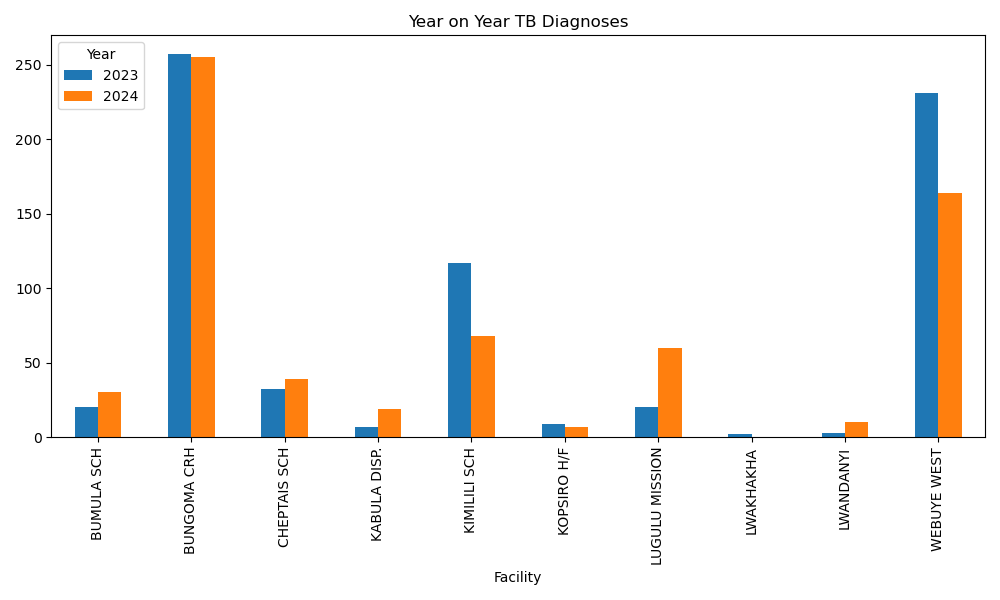
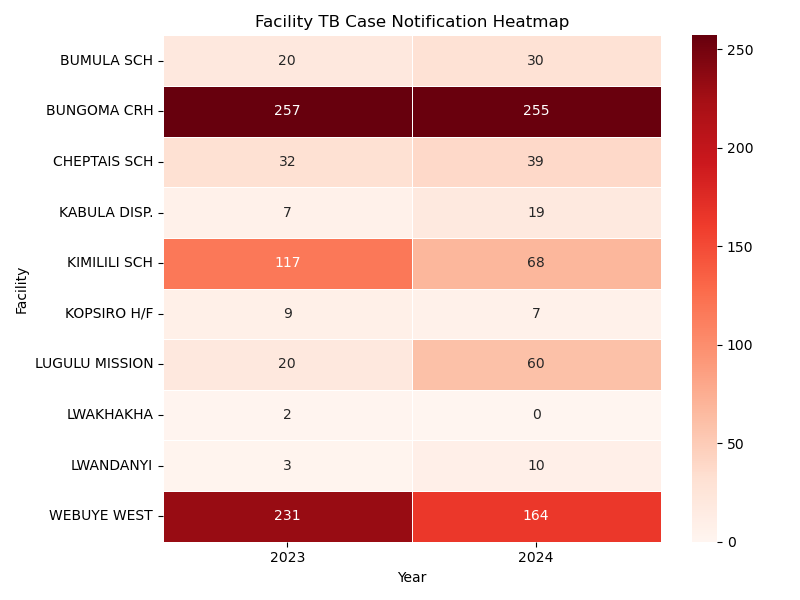
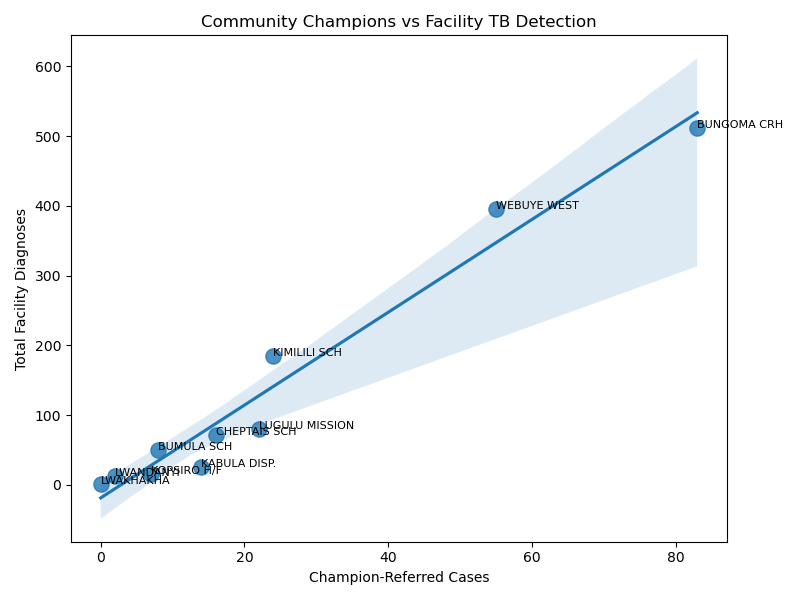
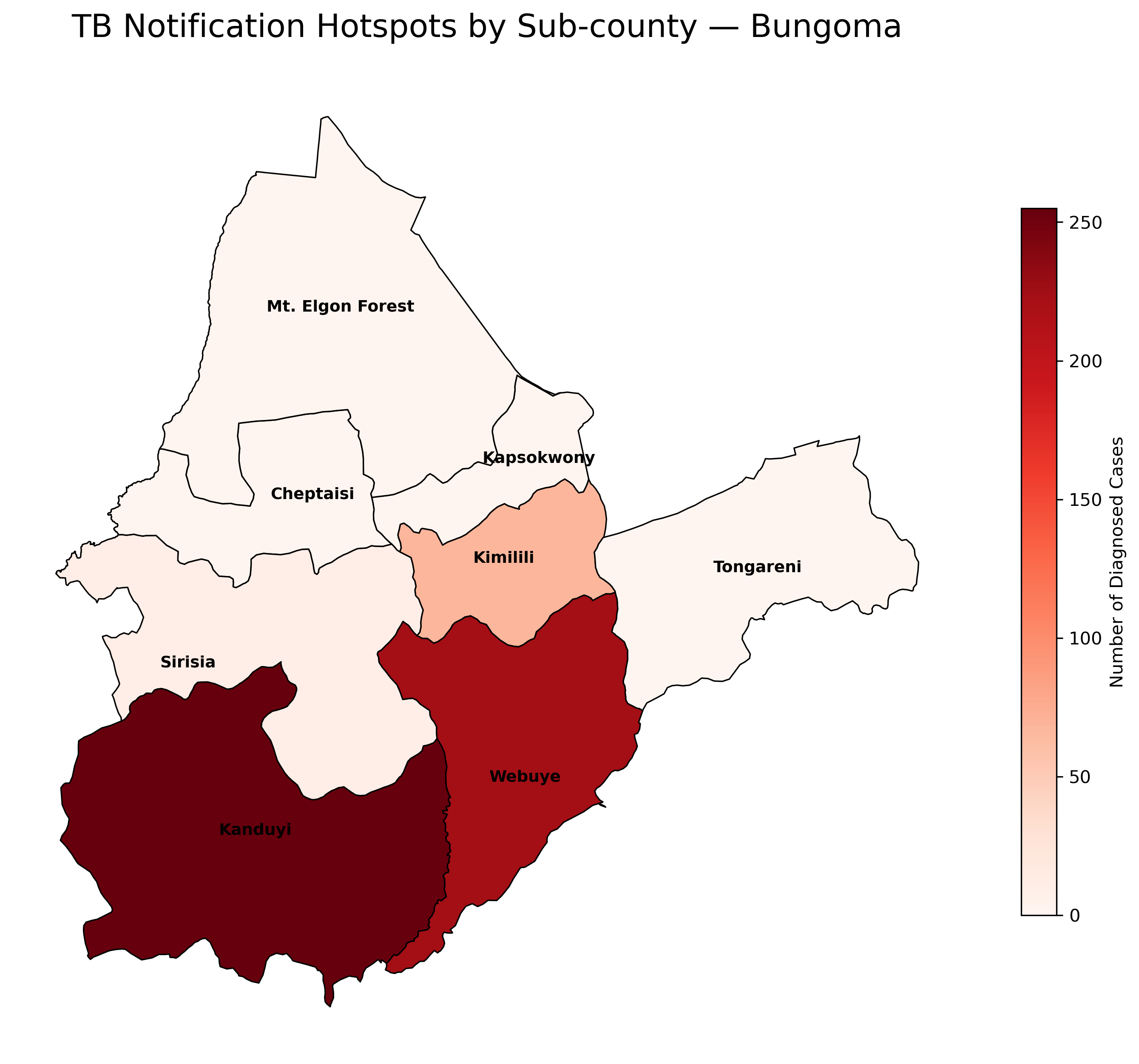
Figure: CFI implementation evidence visuals (facility trend, heatmap, champion contribution elasticity, and hotspot map).

We gratefully acknowledge the Stop TB Partnership's TB REACH initiative for supporting this research/program through a Wave 11 grant. The project was designed to increase Participation, Accountability, Non-discrimination, Empowerment, Linkage and Sustainability among vulnerable and marginalized populations affected by TB in Bungoma Kenya, and was supported by funding from Global Affairs Canada. Stop TB Partnership is hosted by UNOPS.
Language note: This brief applies people-centered, non-stigmatizing language in line with Stop TB Partnership guidance.










Preview and download workflow for this brief is available in Impact > Reports & Evidence.